Nabízíme širokou škálu ortodontického materiálu a výrobků z oblasti estetické stomatologie
Nabízíme širokou škálu ortodontického materiálu a výrobků z oblasti estetické stomatologie
Odborné články
Correction of a Canted Lower Incisal Plane
- VOLUME 40 : NUMBER 09 : PAGES (555-559) 2006
- MICHAEL DELUKE, DDS, MDS
- FLAVIO URIBE, DDS, MDS
- RAVINDRA NANDA, BDS, MDS, PHD
A cant of the mandibular incisal plane can be difficult to recognize in a patient with a unilateral skeletal crossbite due to a lateral CO-CR shift, especially if the patient has an impinging deep bite. A differential diagnosis between an incisal cant and an occlusal cant is of primary importance, because while the former can be corrected with well-controlled, determinate force systems, the latter usually requires controlling the eruption of the buccal segments in growing individuals or, in adults, can often be resolved only through ortho-gnathic surgery.
This article demonstrates an effective method by which an incisal cant can be leveled to achieve an ideal occlusion with a symmetrical overbite.
Case Report
A 12-year-old male in the permanent dentition presented with the chief complaint of an anterior crossbite. He had a Class II, division 1 subdivision right malocclusion with a narrow maxilla (Fig. 1). The maxillary midline coincided with the facial midline, but the mandibular midline had shifted 3mm to the right, resulting in a unilateral crossbite. The patient also showed a slight cant of the lower incisor segment.
{kind=link}
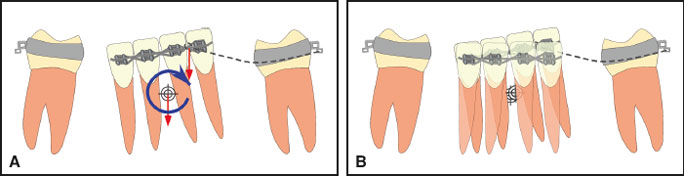
Comprehensive orthodontic treatment was begun with rapid palatal expansion of the maxillary arch. Full fixed appliances were then bonded for leveling and alignment, with a continuous .014" nickel titanium wire placed in the lower arch. At that point, a significant mandibular cant became obvious (Fig. 2). One month later, an .016" x .022" stainless steel archwire was sectioned between the canines and incisors on both sides, and an .017" x .025" CNA Beta Titanium cantilever wire was bent down into the mucobuccal fold on the left side, from the first molar auxiliary tube to the main archwire between the central and lateral incisors (Fig. 3). This point of attachment, off-center from the lower midline, was selected to obtain not only an intrusive force, but a moment around the center of resistance of the anterior segment (Fig. 4). To prevent any spaces from opening, the segments from the lower right first molar to the left lateral incisor and from the lower left first molar to the left canine were ligated together.
{kind=link}
{kind=link}
{kind=link}
After 10 weeks, with no reactivation of the cantilever, a significant amount of intrusion and rotation of the anterior segment had been achieved, but the incisal cant was not fully corrected. The cantilever was then moved to the distal end of the anterior segment, thus increasing the magnitude of the moment in relation to the center of resistance of the anterior teeth (Fig. 5).
{kind=link}
Once the lower anterior segment had been corrected, a vertical discrepancy between the incisors and the left canine became evident. A similar cantilever with an intrusive force was then attached to the lower left canine, and an .016" x .022" stainless steel archwire was inserted from the lower right first molar to the lower left lateral incisor to maintain the correction of the incisal cant (Fig. 6).
{kind=link}
When the lower arch was almost completely leveled, a continuous .017" x .025" CNA archwire was placed in the lower arch, and a vertical seating elastic was used on the right side to extrude the lower canine and premolar and finish the correction of the incisal cant (Fig. 7). An .017" x .025" stainless steel wire was placed in the upper arch to minimize any extrusion of the maxillary teeth. Detailing was completed with esthetic wire bends (Fig. 8).
{kind=link}
{kind=link}
The total treatment time was 23 months (Fig. 9).
{kind=link}
Discussion
Figure 10 shows another patient with a similar lower incisor cant. The same mechanics were applied, using a cantilever to intrude the lower left anterior segment and subsequently intrude the lower left canine.
{kind=link}
Segmented arches and cantilevers can effectively correct problems, such as a canted incisal plane, that would be difficult to resolve by any other means. By understanding and controlling side effects, the clinician can achieve an ideal result in a relatively short time.