Nabízíme širokou škálu ortodontického materiálu a výrobků z oblasti estetické stomatologie
Nabízíme širokou škálu ortodontického materiálu a výrobků z oblasti estetické stomatologie
Odborné články
Slow Maxillary Expansion with Nickel Titanium
- VOLUME 33 : NUMBER 08 : PAGES (431-441) 1999
- ROBERT MARZBAN, DDS
- RAVINDRA NANDA, BDS, MDS, PHD
Correction of a transverse discrepancy usually requires expansion of the palate by a combination of orthopedic and orthodontic tooth movements. Initially, transverse forces will tip the buccal segments laterally. With proper appliance design, 3rd-order moments will induce bodily translation. If the force is strong enough, separation occurs at the maxillary suture. The amount of orthopedic vs. orthodontic change depends greatly on the patient's age. Normal palatal growth is nearly complete by age 6, and increasing interdigitation of the suture makes separation difficult to achieve after puberty.
The rationale for sutural expansion, assuming the problem is diagnosed early enough, is twofold. First, a skeletal discrepancy should be treated by orthopedic correction whenever possible. Second, dental compensation by buccal translation or tipping is undesirable, because the thin layer of bone covering the roots of the buccal segments is prone to penetration.
The objective of rapid palatal expansion is to reduce undesirable orthodontic tooth movement and tipping while producing enough force to overcome the tendency of the anchor teeth to move, thereby maximizing the orthopedic response by causing separation at the suture. RPE appliances require frequent activations and generate heavy forces--as much as 2-5kg per quarter-turn, with accumulated loads of more than 9kg.
Although sutural separation is relatively easy to obtain with RPE, implant data indicate that sutural expansion accounts for only about 50% of the overall expansion. In more than 30% of Krebs's sample of 23 patients, sutural expansion was less than onethird of the total expansion.
Buccal tipping, even of the amount produced by RPE, is highly unstable and prone to relapse quickly. According to Haas, fixed retention after RPE can virtually eliminate sutural relapse. However, using the same split-palate-expanding appliance, Krebs found that the distance between implants in the hard palate and infrazygomatic ridge decreased during retention by 10-15%. This relapse was found to occur as late as four or five years after fixed retention.
Rationale for Slow Maxillary Expansion
Increases in arch width obtained through slow palatal expansion procedures are generally thought to result in an orthodontic response with little, if any, orthopedic component. By contrast with RPE, only 450-900g of force is generated, which may be insufficient to separate a progressively maturing suture.
In animal studies, however, slow expansion procedures have demonstrated orthopedic effects comparable to those of RPE. Histologic examination suggests that sutural separation does occur, but at a rate that maintains the integrity of the maxillary sutures by allowing for bone remodeling. Clinical studies of human patients in the deciduous or early mixed dentition substantiate these findings: maxillary archwidth increases ranged from 3.8mm to 8.7mm with slow expansion of as much as 1mm per week, using 900g of force.
Zimring and Isaacson suggest that "the optimum rate of activation would be one whereby additional loads are added at close to the same rate that the facial skeleton can respond by physiological movement". Storey recommends slow expansion at .5-1mm per week to allow for "physiological sutural adjustments", which elicit less trauma and a greater repair response compared to rapid expansion. Ekstrom reports that slowly expanded sutures become well organized in 30 days and are well established with mineralized tissue by three months.
Slow expansion has been found to promote greater postexpansion stability, given an adequate retention period. Furthermore, in a comparison of slow expansion (with a Quad Helix) and RPE, Zachrisson concluded that periodontal breakdown on the buccal aspects of posterior teeth occurred infrequently in both groups, but that the few patients who exhibited some attachment loss were mostly in the RPE group.
In addition to these biological benefits, slow expansion techniques offer a number of clinical advantages. An ideal slow expansion appliance requires minimal adjustment throughout its use, but permits easy adjustment when necessary. It delivers a constant physiologic force until the required expansion is obtained. The appliance is light and comfortable enough to be kept in place for sufficient retention of the expansion. Prefabrication eliminates extra appointments for impressions and the time and expense of laboratory fabrication.
The present article describes such an expansion appliance.
Nickel Titanium Palatal Expander
The nickel titanium expander generates optimal, constant expansion forces (Fig. 1). Its central component is fabricated from a thermally activated nickel titanium alloy. The rest of the appliance, including the anterior arms, is made of stainless steel. The expander may be used simultaneously with conventional fixed appliances, requiring only the addition of lingual sheaths on the molar bands.
{kind=link}
The nickel titanium component has a transition temperature of 94ºF. At room temperature, the expander is too stiff to bend for insertion. Chilling the expander softens the central component, allowing easy manipulation. Once placed, the expander warms to body temperature, stiffens, and begins to return to its original shape. A 3mm increment of expansion exerts only about 350g of force, and the nickel titanium alloy provides relatively uniform force levels as the expander deactivates.
The expander is available in sizes from 26mm to 44mm. In most cases, the simplest way to determine the appropriate size is to measure the mandibular intermolar width at the central fossae (Fig. 2). Since the mesiolingual cusps of the maxillary molars should occlude in these fossae, expansion to the mandibular intermolar width will provide optimal occlusion (Fig. 3). If the mandibular molars are lingually inclined as a dental compensation for a skeletal posterior crossbite, as often occurs, it is appropriate to add another 1-2mm to the expansion requirement. In any case, 2-3mm should be added for overexpansion (Fig. 4). If more than 8mm of expansion is needed, two expanders must be used in succession.
{kind=link}
{kind=link}
Clinical Technique
1. Select the appropriate size expander, based on measurement of the study casts.
2. Adjust the anterior arms of the expander as needed.
3. Wrap the central component with moist gauze (Fig. 5), and place the expander in the freezer.
{kind=link}
4. Determine the appropriate band sizes, and fit bands (with lingual sheaths) as usual (Fig. 6).
{kind=link}
5. Cement the bands with a dual- or light-cured cement.
6. Remove the expander from the freezer, and with the gauze still in place, slide the inserts into the molar sheaths.
7. Remove the gauze from the expander.
An alternative method involves assembly of the expander and bands extraorally, and cementation as one unit. This procedure is preferable where access to the palate is restricted and insertion may be difficult. The drawback of this method is that it requires rapid band placement and cementation as the expander warms to oral temperature.
Many options are available for cooling the expander prior to insertion (Fig. 7). The expander may be put in a freezer or cooled with gel freeze packs until ready for placement. Alternatively, a refrigerant spray such as ethyl chloride or tetrafluoroethane can be used immediately prior to insertion to chill the expander, which is then wrapped in gauze and placed in the mouth. The moist gauze insulates the cooled expander from body temperature, thereby increasing the working time.
{kind=link}
If the molars are rotated, the anterior arms of the expander may not initially contact the buccal segments. It is usually not necessary to adjust these arms until some derotation has occurred.
The rate of expansion will depend on the age of the patient. Patients in the primary or early mixed dentition can be expanded in one to two months, depending on the severity of the case. Expansion in adolescents can take as long as three months, and even longer expansion and retention times should be expected in adults. The retention period should be 50-100% of the expansion time.
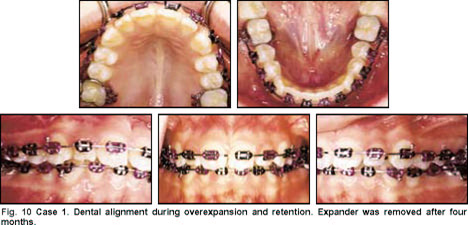
Case 1
A prepubertal female, 10 1/2 years of age, presented with a constricted, sigmoid-shape maxillary arch with moderate to severe crowding (Fig. 8). Both maxillary molars were rotated mesial-in, the right molar more severely. The resultant loss of arch length created an asymmetrical Class II molar relationship with the right second premolar blocked palatally. Both maxillary canines were erupting ectopically. Overbite and overjet were 1mm each.
{kind=link}
The mandibular intermolar width was 31mm at the central grooves, while the maxillary intermolar width was 28mm at the mesiolingual cusps. A size 34 expander was selected, based on the mandibular intermolar width plus 3mm for overcorrection.
A chin cup was prescribed for the first month to control the vertical dimension during expansion. After one month, 3mm of transverse correction had been achieved (Fig. 9). The expander was left in place for three more months of overcorrection and retention, while alignment and leveling of the dentition were carried out (Fig. 10). The arches were then leveled with rectangular wires. Treatment was completed shortly thereafter with minor finishing (Fig. 11).
{kind=link}
{kind=link}
{kind=link}
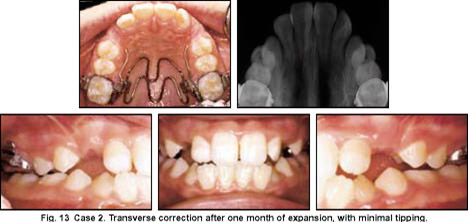
Case 2
An 11-year-old postpubertal female presented with a slightly crowded dentition and a Class I occlusion (Fig. 12). The left posterior segment was in crossbite. The overjet and overbite were 2mm each.
{kind=link}
The mandibular intermolar width measured 36mm; the maxillary molars spanned 33mm. A size 38 expander was selected. After four weeks, the transverse discrepancy had been corrected (Fig. 13). In four more weeks, the desired over-expansion was complete (Fig. 14). The expander was left in place for another two months for retention (Fig. 15).
{kind=link}
{kind=link}
{kind=link}
Treatment of the remaining dentition was delayed until the primary mandibular second molars were mobile and the maxillary canines had begun to erupt. At that time, brackets were placed for simple alignment and finishing.
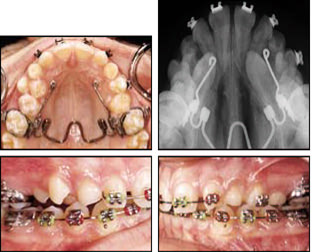
Case 3
A 13-year-old male presented with a Class I molar occlusion, bilateral impacted maxillary canines, and a mild posterior transverse discrepancy (Fig. 16). Only minimal expansion was needed in this case; it was more important to establish proper 3rd-order inclination of the molars and to obtain sufficient posterior anchorage to extrude the impacted maxillary canines.
{kind=link}
A Nitanium Palatal Expander 2 was used to allow 1st- and 3rd-order adjustments to be made as necessary (Fig. 17). The central nickel titanium component of this expander is attached to .036" stainless steel loops, which may be adjusted in any dimension or orientation.
{kind=link}
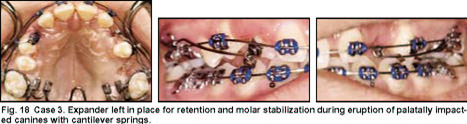
Proper buccal overjet was obtained and held for two months. The anterior steel arms were then cut off to allow the surgeon to have clear access for the canine exposure. The expander was maintained for anchorage while the canines were erupted with III Titanium (CNA) cantilever springs (Fig. 18).
{kind=link}
Discussion
Occlusal x-rays will seldom show palatal separation during slow expansion procedures. The gradual rate of expansion maintains tissue integrity and elicits a physiologic response that allows bone deposition along the suture to keep pace. Consequently, an unsightly midline gap can be avoided, and the arch length gained can be used to align ectopic canines and premolars, as shown in Cases 1 and 3.
Orthodontic tooth movement and buccal tipping occur initially, but are kept to a minimum. Third-order moments generated by the expander soon upright the molars and provide stable, orthopedic maxillary expansion.
As in any expansion procedure, overexpansion is necessary to compensate for the tendency of the posterior teeth to return to their pretreatment axial inclinations. The best benchmark, therefore, is the 3rd-order inclination of the posterior teeth. Once the transverse discrepancy has been corrected, the expander should be kept in place long enough to correct any buccal tipping that occurred earlier in the expansion process. The mandibular buccal segment will gradually upright itself, eliminating dental compensations from the preexisting crossbite.
In patients with excessive lower facial height, vertical control is essential. A chin cup, used for a short period of time, is an excellent way to control bite opening during expansion. Highpull headgear may be used for a longer period to control the vertical eruption of the maxillary molars while correcting a Class II molar relationship.
Conclusion
The nickel titanium expander provides a viable alternative to rapid expansion for correction of transverse discrepancies. Incorporation into an existing fixed appliance eliminates a separate laboratory phase and extra appointments for delivery, impressions, adjustments, and rebanding of the molars after removal. The buccal molar attachments are free for use with intrusion arches, utility arches, wire segments, extraoral appliances, or comprehensive fixed appliances. The expander is not cumbersome or uncomfortable and thus can be kept in place for retention and anchorage, even while other procedures are being performed.